
A physician I know recently said this out loud, to no one in particular, after a long day: "I don't want another peer-to-peer call with insurance to justify my care."
Sit with that word for a moment. Justify.
More than a decade of training. Board certifications. A patient in front of you that you know — their history, their labs, their family, the three medications they've already tried. And at the end of the day, you still have to pick up the phone and justify your clinical judgment — to a clinician on the other end who is often defending a denial an algorithm produced in 1.2 seconds.
That sentence — I don't want another peer-to-peer call to justify my care — is not an outlier. It is the single most common feeling in American medicine right now. And the data underneath it is starker than most physicians realize.
In the first three issues of The Agentic Practice, I wrote from the operator's chair. The system squeezing independent practices from every direction. The twelve-portal ritual your front desk runs before every Thursday. The 47 faxes sitting in an inbox before the first patient walks in. This issue is different. This one is written from the chair across from the patient.
Table of Contents
- Why is the wheel getting heavier?
- What does "I can only go so fast" actually mean?
- Why don't physicians open the denial letters anymore?
- What is the system actually saying?
- What happened to the off-ramp?
- Why did the existing solutions fail?
- What is the work for?
- What does the wheel cost?
- Why is this the independent practice's fight?
- Frequently Asked Questions
Why is the wheel getting heavier?
A different physician, in a different conversation, said something that stuck with me: "I'm on a hamster wheel of fee-for-service. I can only go so fast." That's the diagnosis — the most accurate description of American outpatient medicine I've heard this year.
Fee-for-service was built on a simple trade: more patients through the door, more revenue. But Medicare physician payment has dropped 33% in inflation-adjusted terms since 2001, while practice costs rose 59%. Commercial and Medicaid follow Medicare down. So the volume goes up just to keep the paycheck level.
Then documentation layered on top — EHRs, quality reporting, MIPS, patient messages — consuming nearly an hour of administrative work for every hour of patient care. Then came the layer that broke the system: justification. Not documentation for care. Documentation about care, directed at payers, demanding that the physician prove, defend, and re-prove every clinical decision. Prior authorization, denial appeals, medical necessity letters — none of this existed at this scale twenty years ago. All of it sits on top of a wheel that was already spinning too fast.
That's not burnout. That's architecture.
What does "I can only go so fast" actually mean?
This is the most universal physician sentence I've heard. Every specialty. Every practice size. Every payment model. The physician running behind at 10:30am isn't behind because they're slow. They're behind because the day was never built for the physician — it was built for the clicks.
The sentence "I can only go so fast" isn't about the hour after clinic. It's about the hour during clinic — the one where the physician is sitting across from a patient, trying to listen, trying to examine, trying to think — while also clicking through problem lists, reconciling medications, charting to the quality measure, and mentally drafting a note that will survive chart review. Both feel it.
Ambient AI scribes were the industry's answer. And they helped, partially. The 2025 AMIA TrendBurden survey found 83.1% of physicians still finish work later than desired because of documentation. Scribes compress that number, but don't eliminate it. Because documentation was never the full burden. Review is.
Every AI-generated note still requires a physician signature, and that signature carries liability. We experienced this directly at Valley Diabetes & Obesity. During a routine visit, an ambient AI system misattributed parts of the conversation — placing patient statements into the physician's voice and altering clinical context. The error was caught during review, but the implication was clear: the physician remains fully accountable for every word in the chart, regardless of how it was generated. In a large health system, that risk is distributed. In an independent practice, it sits entirely with the physician signing the note.
So the physician runs faster. Sees the patient, reviews the AI note, corrects the AI note, signs the AI note, moves to the next room. The pace compresses. The weight doesn't lift. It just gets redistributed across more clicks per hour.
"I can only go so fast" is a boundary statement from a physician who has discovered that the ceiling on their day is not their stamina — it's the number of interruptions, verifications, and reviews the system demands between them and the next patient.
Why don't physicians open the denial letters anymore?
"I don't want to open all these denial letters." This is a different kind of exhaustion. Not the exhaustion of too many tasks. The exhaustion of tasks that feel pointless.
Prior authorization and denial management are the two workflows in American medicine where the physician's clinical expertise is most directly contested. An average physician now completes 39 prior authorizations per week. Staff and physicians spend 13 hours on them. And when a PA is denied, or a claim comes back rejected, the physician has two options: appeal, or let it go.
89% of physicians in the AMA's 2024 survey said prior authorization contributes to their burnout. 93% said it delays patient care. 82% said patients commonly abandon treatment because of it. 29% reported it caused a serious adverse event for a patient in their care.
These aren't process complaints. These are physicians saying: the paperwork between me and my patient is now producing clinical harm. And when the denial arrives — often in a 1.2-second algorithmic response, with a boilerplate reason that may or may not match the patient's actual chart — the physician has to decide whether to fight it. Compose the appeal. Schedule the peer-to-peer call. Defend, in writing and by phone, the same decision they already made with the patient in the room.
The physician sentence for this isn't anger. It's avoidance. I don't want to open all these denial letters. Every envelope contains another demand to defend care that was already provided, already documented, already correct.
What is the system actually saying?
There is another dimension of this that physicians feel but rarely name out loud. Every denial is the payer saying we don't think this care was necessary. Every downcoded claim is the payer saying we don't think you did the work you claim you did. Every prior authorization hoop is the payer saying we don't think your patient is as sick as you think they are, or that they deserve what you're recommending.
And the patient absorbs the cascade. When their prior auth is denied for the third time, when their medication is downgraded to step therapy, when they wait three weeks for an imaging approval — they lose trust in the physician who seems unable to deliver the care that was promised. Even though none of it is in the physician's hands.
In the 2024 AMA survey, physicians who don't appeal prior authorization denials were asked why. Sixty-seven percent said it was because past experience told them appealing wouldn't work. Read that sentence again.
Two-thirds of American physicians have stopped fighting back, because the system has taught them that the last hour of their day is better spent on anything else. That is what justified care looks like in 2026.
But here's what makes all of this accelerate: the people who were absorbing the weight are leaving. A strong MA, a tenured biller, a prior auth specialist who knows the intricacies of each payer — which plan needs a letter of medical necessity, which formulary requires step therapy documentation, which reviewer will approve on the first call — they absorb the justification demands before they reach the physician. Billing turnover in small practices runs at 30% annually. MGMA reports 92% of practices have hired or reassigned staff solely to handle prior authorization volume. When that specialist leaves, the PA queue doesn't pause. It compounds on the physician's desk. The same forces that break the physician break the team that was protecting them. It's a circuit that feeds itself.
What happened to the off-ramp?
There was supposed to be a way off the wheel. Value-based care. A 400-patient panel instead of 2,000. Depth instead of throughput.
For large systems, it arrived. For independent practices, it didn't. And concierge medicine — the other off-ramp — isn't a choice for practices serving Medicare, Medi-Cal, and fixed-income patients. A $2,000 membership fee solves the physician's burnout by pricing out the patients who most need the continuity.
So the physician who stayed independent specifically to practice differently is still on the same wheel. I'll dedicate a future edition to why VBC didn't arrive for small practices, and what comes next.
Why did the existing solutions fail?
Every layer that was supposed to reduce burden has instead redistributed it.
Electronic health records digitized documentation, but they also multiplied the number of required fields, clicks, and compliance checkpoints. The work didn't disappear — it became structured, tracked, and expanded.
Ambient AI scribes compress documentation time, but they don't eliminate responsibility. Every note still requires physician review, correction, and signature. The liability remains fully human, even when the draft is machine-generated.
Staffing was the buffer. Experienced billers and prior authorization specialists absorbed payer friction before it reached the physician. But with turnover approaching 30% annually in small practices, that buffer is unstable. When it breaks, the work does not disappear — it moves upstream to the physician.
Value-based care was supposed to be the off-ramp. For large systems, it was. For independent practices, it remains structurally out of reach. Attribution models, reporting requirements, and capital constraints prevent most small practices from fully participating.
None of these solutions remove the need to justify care. They only redistribute it.
What is the work for?
Every issue of this newsletter so far has been about what's broken and what we're building to fix it. This issue is about why that matters.
Because the operational improvements are real, but they are not the point. The point is giving physicians and operators room to practice — against a system that was never going to be kind to them, against the slow erosion of the reason anyone went into medicine in the first place.
That's what the phrase bring joy back to practicing medicine actually means. Not a mindfulness program. Not a wellness app. The joy didn't leave because physicians stopped caring. It left because the system made caring the thinnest part of the day.
Bringing it back does not require reforming CMS or winning a policy battle with payers. It requires removing the work that sits between the physician and the patient — not compressing it, not delegating it, but eliminating it from the physician's workflow entirely.
The current generation of tools stops short of that. They assist the physician. They still require the physician to initiate, review, correct, and approve every step.
Agentic systems operate differently. They execute workflows end-to-end — initiating prior authorizations, tracking payer requirements, generating and submitting documentation, and managing follow-through — without requiring the physician to drive the process. The shift is architectural: the physician is no longer the operator of the administrative layer. The system is.
And it's the first technology in thirty years that can do this at the scale a small practice can afford — without asking permission from seven systems that weren't built to coordinate. That's what we're building at Agentman. That is what makes this the first real off-ramp.
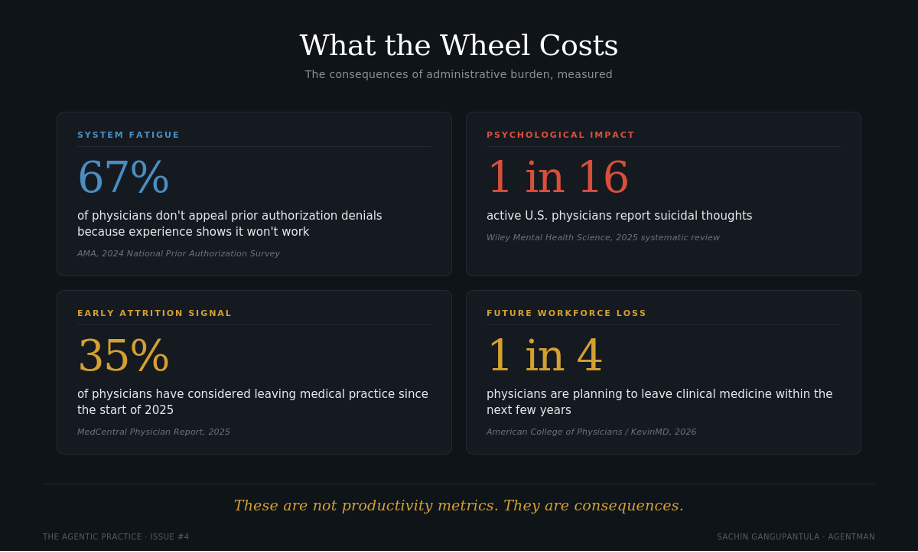
What does the wheel cost?
From friction to exit — how administrative burden translates into physician loss. When you quantify that weight, the pattern becomes hard to ignore:
| Signal | Data Point | Source |
|---|---|---|
| System fatigue — Physicians who don't appeal prior authorization denials because experience shows it won't work | 67% | AMA, 2024 National Prior Authorization Survey |
| Psychological impact — Active U.S. physicians who report suicidal thoughts | 1 in 16 | Wiley Mental Health Science, 2025 systematic review |
| Early attrition signal — Physicians who have considered leaving medical practice since the start of 2025 | 35% | MedCentral Physician Report, 2025 |
| Future workforce loss — Physicians planning to leave clinical medicine within the next few years | 1 in 4 | American College of Physicians / KevinMD, 2026 |
These are not productivity metrics. They are consequences.
These are not separate signals. They are the same system, expressed at different stages. Physicians don't leave medicine because the work is too hard. They leave because the work has become disproportionately about defending work they already did for a patient they already know.
Why is this the independent practice's fight?
Employed physicians cannot redesign their own admin layer. The health system owns the workflow, the vendor contracts, and the IT roadmap. A physician inside a 500-provider system who wants to change the workflow has to convince seven decision-makers and wait two budget cycles. Most of the time, they don't get to try.
Independent practices don't have that problem.
A three-physician practice can deploy an agent on a Tuesday. A ten-physician practice can redesign its prior auth workflow in a month. The sovereignty to move — to decide, fund, and implement inside your own four walls — is the one structural advantage independents still hold. And for the first time in thirty years, there is a technology that matches the size of that sovereignty.
Physicians didn't train for more than a decade to run a faster wheel. They trained to practice medicine. The wheel doesn't stop on its own. Someone has to build the off-ramp.
The system won't fix itself. Independent practices are the last place where it still can — and the last place where it will.
Frequently Asked Questions
What does "justify my care" mean in the context of physician burnout?
"Justify my care" is the phrase a physician used to describe peer-to-peer calls with insurers. It captures a third administrative layer that barely existed twenty years ago: documentation about care directed at payers, demanding that physicians prove, defend, and re-prove clinical decisions through prior authorization forms, medical necessity letters, denial appeals, and peer-to-peer calls. It is distinct from documentation for care — the chart note — which has always been part of medicine.
Why do 67% of physicians no longer appeal prior authorization denials?
According to the AMA's 2024 National Prior Authorization Survey, 67% of physicians who don't appeal cite past experience telling them appealing wouldn't work. The non-appeal rate is the clearest signal that the denial feedback loop has broken: two-thirds of American physicians have stopped fighting back because the last hour of their day is better spent on anything else.
How are ambient AI scribes different from agentic AI in healthcare?
Ambient AI scribes listen to the patient encounter and draft clinical notes. The physician still reviews, corrects, and signs every note, and the liability remains fully human. Agentic AI executes administrative workflows — prior authorizations, denial appeals, claims follow-up, payer communication — end-to-end, without requiring the physician to drive each step. Ambient AI compresses documentation time. Agentic AI removes the administrative layer from the physician's workflow entirely. Both can coexist: ambient captures the encounter, agentic acts on it downstream.
Why hasn't value-based care worked for independent practices?
Value-based care arrived for large health systems that could absorb attribution models, reporting requirements, and the capital investment required to manage risk-based contracts. For independent practices, the administrative complexity of multiple VBC contracts, the cost of care management infrastructure, and the difficulty of reaching attributed-lives thresholds have kept it structurally out of reach. The physician who stayed independent specifically to practice differently is still on the same fee-for-service wheel.
What can an independent practice do today to reduce the burden of justifying care?
Three actions are available now. First, measure the actual weekly volume of prior authorizations, denials, appeals, and peer-to-peer calls flowing through the practice, and note how much reaches the physician versus staff. Second, identify the denial categories the practice has stopped appealing — that is where recoverable revenue is sitting. Third, evaluate agentic AI systems that execute prior authorization and denial management workflows end-to-end, rather than assistive tools that only speed up individual steps. The test is simple: does the system execute the workflow, or does it just help the physician execute it faster?
If you or a physician you know is struggling, the Physician Support Line is free, confidential, and staffed by psychiatrists: 1-888-409-0141. The Dr. Lorna Breen Heroes' Foundation also provides resources specifically for clinicians.
If this issue resonates — or if there's a sentence you want to push back on — I'd value hearing from you in the comments. The next edition returns to the operator's chair, with field notes from Valley Diabetes & Obesity on what's working and what isn't.


