The most important work in your practice happens two to three days before the patient ever walks in — and nobody outside the front desk sees it.
Someone on your team pulls up Thursday's schedule on a Tuesday afternoon. And the ritual begins. Open browser. Navigate to the first payer portal. Enter credentials. Wait for the two-factor code. Search for the patient. Click through three screens to confirm coverage is still active. Copy the details into the chart. Close the tab. Repeat for the next payer. And the next.
Twelve portals across Medicare, Medicaid, commercial plans, and IPA networks. Different logins. Different interfaces. Different quirks. One portal times out after five minutes of inactivity. Another requires a password reset every 30 days. A third displays coverage data in a format that doesn't match what your billing system needs.
If you run a practice, you already know this ritual. You might even know it so well that you've stopped noticing how fragile it is — and how much of your revenue depends on one person doing it right, every time. The U.S. healthcare industry spends $43 billion a year on this single workflow — and most of it is still done manually.
Table of Contents
- What Does Eligibility Verification Actually Look Like in an Independent Practice?
- Why Can't Your EHR Handle Eligibility Verification?
- Why Is Eligibility Verification a Continuous Process — Not a One-Time Check?
- What Are the Real Costs of Manual Eligibility Verification?
- How Did One Independent Practice Eliminate Portal Logins Entirely?
- Why Does This Matter Beyond a Single Practice?
- Frequently Asked Questions
- Key Takeaways
What Does Eligibility Verification Actually Look Like in an Independent Practice?
Eligibility verification in an independent practice is a ritualized, portal-by-portal manual process where a dedicated staff member logs into as many as 12 separate payer portals — each with different credentials, interfaces, and quirks — to confirm coverage, copays, deductibles, and PCP assignment for every patient on the upcoming schedule. This process typically begins two to three days before each appointment day.
The workflow is invisible to anyone outside the front desk, but it is the operational engine that determines whether a practice's schedule runs smoothly or falls apart. A staff member pulls up Thursday's schedule on a Tuesday afternoon and the ritual begins: open browser, navigate to the first payer portal, enter credentials, wait for two-factor authentication, search for the patient, click through multiple screens to confirm coverage, copy the details into the chart, close the tab, and repeat.
Each of the 12 portals across Medicare, Medicaid, commercial plans, and IPA networks presents different challenges. One portal times out after five minutes of inactivity. Another requires a password reset every 30 days. A third displays coverage data in a format that doesn't match the practice's billing system.
The fragility of this workflow is its most dangerous feature. When the person who runs verifications calls in sick or gives two weeks' notice, all of the institutional knowledge — which portal needs which workaround, which IPA requires a phone call, which Medicaid plans need manual lookup — walks out the door. Thursday's schedule starts falling apart before anyone realizes why.
Why Can't Your EHR Handle Eligibility Verification?
Every EHR includes a built-in eligibility check, but these checks consistently fall short of what front-desk staff actually need to prevent denials and protect practice revenue. EHR eligibility checks confirm whether coverage is active or inactive — they do not extract the financial and assignment details required to bill correctly and set patient expectations.
Every practice manager has tried the EHR's eligibility tool. And every practice manager knows where it fails. The system can't reconcile mismatched patient data. It can't resolve Medicaid eligibility. It doesn't recognize local IPA plans.
The real gap is what the EHR check doesn't even attempt. Staff need to extract the patient's current copay amount, determine how much of the deductible has been met, and confirm out-of-pocket maximum status. They need to verify whether the practice is in-network or out-of-network for that specific plan. They need to confirm that the patient is actually assigned to the correct PCP — because if they're not, the practice won't get paid regardless of what the coverage says.
For Medicare patients, the stakes are even higher. If a patient has switched from Original Medicare to a Part C Medicare Advantage plan, the eligibility check needs to surface that change so staff can collect the new insurance information before the visit. Miss that transition, and the practice bills the wrong payer entirely.
This is why eligibility verification demands a dedicated person — not because the verification itself is complex, but because the information required goes far beyond what any EHR eligibility check returns. That person isn't just verifying. They're triaging the entire schedule: flagging expired coverage, identifying reassigned patients, calling patients before appointments, and filling open slots from the waitlist when cancellations occur.
Why Is Eligibility Verification a Continuous Process — Not a One-Time Check?
Eligibility verification is not a single pre-visit event. It recurs at a minimum of three touchpoints per patient encounter — at scheduling, 48 to 72 hours before the visit, and at check-in — and extends through billing, referrals, and ongoing chronic care management. The industry best practice of three verification checkpoints per encounter generates 90 to 120 verification events daily for a practice seeing 30 to 40 patients.
The verification cycle begins before a patient ever sets foot in the practice. When a new patient calls and asks, "Does Dr. G take my insurance?" — that is an eligibility question. The front desk needs to answer it before offering an appointment slot. If they can't verify quickly, that patient calls the next name on their list, and the practice loses a new patient without ever knowing it.
Verification touchpoints across the patient journey:
| Touchpoint | What's Verified | Risk If Skipped |
|---|---|---|
| Scheduling | Plan active, practice in-network | Lost new patient, wasted appointment slot |
| 48–72 hours before visit | Coverage changes, employer switches, Medicaid redeterminations | Surprise coverage gap at check-in |
| Check-in | Last-chance coverage confirmation, correct copay collection | Incorrect copay, patient friction |
| Billing | Claim built against collected coverage data | Denial, write-off, rework cycle |
| Ongoing (chronic care) | Monthly/biweekly for recurring patients, referrals, prior authorizations | Accumulated revenue leakage |
For chronic disease practices, the cycle never stops. At Valley Diabetes & Obesity, our patients come back every month — sometimes every two weeks. Every visit, every referral, and every prior authorization triggers another eligibility question. Multiply that by a full patient panel, and this single workflow can make or break a practice's cash flow.
In a practice seeing 30 to 40 patients a day, three touchpoints per encounter means 90 to 120 verification events every single day. Across 12 payer portals. Manually. With a team that's also answering phones, checking patients in, and filing prior authorizations. That's not a workflow — it's a staffing crisis disguised as an administrative task.
What Are the Real Costs of Manual Eligibility Verification?
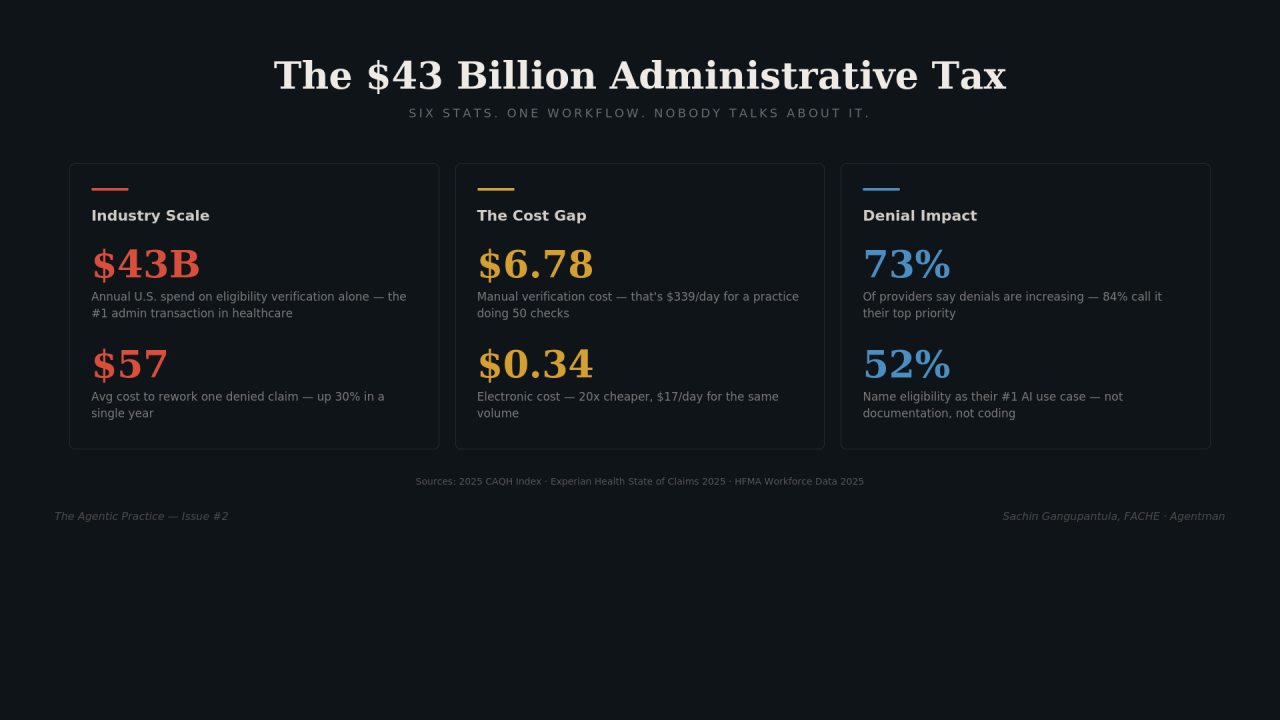
A single manual eligibility verification costs $6.78, compared to $0.34 for a fully electronic verification — a 20x cost gap. For a practice running 50 verifications per day, that translates to $339 daily for manual processing versus $17 automated, or more than $80,000 annually in direct transaction costs alone — before accounting for downstream denials, rework cycles, and lost revenue.
The CAQH Index, the industry's authoritative benchmark for administrative transaction costs, found that spending on eligibility and benefit verification reached $43 billion — representing a 60% increase and the largest share of annual medical administrative spend at 51%.
The cost differential is staggering at every scale:
| Practice Volume | Manual Daily Cost | Automated Daily Cost | Annual Savings |
|---|---|---|---|
| 25 verifications/day | $169.50 | $8.50 | $41,860 |
| 50 verifications/day | $339.00 | $17.00 | $83,720 |
| 100 verifications/day | $678.00 | $34.00 | $167,440 |
These figures capture only direct transaction costs. The downstream impact — denied claims, rework time, lost patients who couldn't get a quick answer at scheduling, and revenue from visits that happened without proper verification — multiplies the true cost significantly.
The industry recognizes this. A full 52% of providers now name eligibility verification as their number one use case for AI — ahead of documentation, coding, and every other administrative function. The pain is clear. The question is whether the solutions being built work for a 3-physician practice or only for a 300-bed hospital.
How Did One Independent Practice Eliminate Portal Logins Entirely?
Valley Diabetes & Obesity deployed a single eligibility verification agent as its first workflow automation — one agent, one task, one measurable outcome — and went from 12 portal logins per verification session to zero, while increasing verification accuracy by running checks automatically at every touchpoint instead of whenever staff could squeeze them in between phone calls.
The decision wasn't driven by a technology exercise. It was driven by the fact that eligibility verification was the single biggest source of daily friction in the practice and the most direct threat to cash flow. When a patient shows up and their coverage has lapsed, one of two things happens: either the practice sees them anyway and absorbs the cost when the claim gets denied, or the front desk has an uncomfortable conversation that damages the patient relationship. Both outcomes are preventable.
The implementation followed a deliberate, single-workflow approach — no big-bang rollout, no IT department required:
- Automated schedule scanning: The agent runs eligibility checks automatically for every patient on the upcoming schedule before staff begins their verification session
- Cross-payer coverage: Checks run across all payer types — Medicare, Medicaid, commercial, and IPA — without portal logins, browser tabs, or two-factor authentication codes
- Financial detail extraction: The agent extracts real-time copay amounts, deductible status, and out-of-pocket maximums — the details front-desk staff need to set patient expectations
- Network and assignment verification: Confirms in-network or out-of-network status for the specific plan and verifies PCP assignment, catching cases where patients have been reassigned without knowing it
- Exception flagging: Cases requiring human judgment — coverage gaps, plan changes, coordination of benefits issues — are flagged and waiting for staff review
The result: the agent handles the volume while humans handle the judgment. When staff is out sick or a new hire is learning the ropes, the verification still runs. The institutional knowledge is no longer locked in one person's head — it's built into the workflow. Verification quality went up, not down, because checks now happen at every touchpoint automatically instead of whenever staff could fit them in.
Why Does This Matter Beyond a Single Practice?
Every independent practice running eligibility verification manually is paying the same $43 billion administrative tax. The 20x cost gap between manual and automated verification is real and documented. Most small practices remain trapped in the portal-login cycle because the existing solutions were built for health systems — not for 3-physician practices with no IT department.
This is the gap in the market. Health systems have dedicated revenue cycle teams, enterprise software budgets, and IT staff to implement and maintain complex integrations. Independent practices have a front-desk person who knows the workarounds for 12 different payer portals — and a revenue model that depends entirely on that person showing up every day.
The approach that worked at Valley Diabetes & Obesity — starting with a single agent, targeting the single highest-impact workflow, measuring one outcome — is designed for this reality. It requires no IT department, no enterprise software contract, and no change management initiative. It replaces the most fragile, most expensive, most revenue-critical manual process with an automated workflow that runs the same way whether your verification expert is at their desk, out sick, or has moved on.
The $43 billion question isn't whether eligibility verification should be automated. It's why independent practices — the ones paying the highest proportional cost — are still the last to get access to the tools that fix it.
Frequently Asked Questions
How many payer portals does a typical independent practice need to access for eligibility verification?
A typical independent practice accesses 12 or more payer portals per verification session, spanning Medicare, Medicaid, commercial insurance plans, and IPA networks. Each portal requires separate login credentials, has a different user interface, and imposes its own quirks — from session timeouts to mandatory password resets. This portal fragmentation is one of the primary drivers of the $43 billion annual industry spend on eligibility verification. MGMA's own survey data confirms this reality — most practices already know they're juggling too many payer portals, with portal overload compounding the eligibility and prior authorization burden that drains staff time and revenue.
What is the cost difference between manual and automated eligibility verification?
Manual eligibility verification costs $6.78 per transaction compared to $0.34 for a fully electronic verification — a 20x gap. For a practice performing 50 verifications per day, manual processing costs approximately $339 daily ($83,720 annually) versus $17 daily ($4,420 annually) for automated checks. These figures represent direct transaction costs and do not include downstream costs from claim denials, rework, or lost patients.
Why can't EHR systems handle eligibility verification adequately?
EHR built-in eligibility checks confirm only whether coverage is active or inactive. They typically cannot extract copay amounts, deductible status, out-of-pocket maximums, in-network vs. out-of-network status for specific plans, or PCP assignment verification. They also struggle with Medicaid eligibility resolution, local IPA plans, and mismatched patient data. These gaps mean staff must still access payer portals directly for the information needed to prevent claim denials.
How many times should eligibility be verified per patient encounter?
Industry best practice requires a minimum of three verification touchpoints per patient encounter: at scheduling (confirming coverage and network status), 48 to 72 hours before the appointment (catching coverage changes), and at check-in (final confirmation and copay collection). For chronic care patients seen monthly or biweekly, verification also triggers with every referral and prior authorization. A practice seeing 30 to 40 patients daily generates 90 to 120 verification events per day.
What happens to the verification process when the primary staff member is unavailable?
When the staff member responsible for eligibility verification is absent — due to illness, vacation, or turnover — institutional knowledge about portal-specific workarounds, payer-specific requirements, and process exceptions leaves with them. The upcoming schedule begins to deteriorate because replacement staff may not know which portals require phone calls, which Medicaid plans need manual lookup, or which IPA networks have non-standard verification procedures. This single-point-of-failure risk is one of the strongest arguments for automation.
Key Takeaways
- The $43 billion problem is real and growing. The U.S. healthcare industry's annual spend on eligibility and benefit verification reached $43 billion, with a 60% increase — the largest share of medical administrative spending at 51%.
- Manual verification costs 20x more than automated. At $6.78 per manual check versus $0.34 electronic, a 50-verification-per-day practice spends over $80,000 annually on direct transaction costs alone.
- EHR eligibility checks don't go far enough. Built-in tools confirm active/inactive status but miss copays, deductibles, network status, and PCP assignment — each a potential denial trigger.
- Eligibility is a continuous process, not a one-time check. Three touchpoints per encounter across 30–40 daily patients means 90–120 verification events per day — a staffing crisis disguised as an administrative task.
- Single-agent automation works for independent practices. Valley Diabetes & Obesity eliminated 12 portal logins per session, improved verification quality, and removed the single-point-of-failure risk — with no IT department required.
The gap isn't whether eligibility verification should be automated. It's that the practices paying the highest proportional cost are the last to get access to the tools that fix it.
→ Subscribe to The Agentic Practice for weekly insights on how independent practices are deploying agentic AI to reclaim time, revenue, and operational resilience.
Originally published in The Agentic Practice — Issue #2, by Sachin Gangupantula FACHE, MBA, CDH-E
Sources: 2025 CAQH Index · Experian Health State of Claims 2025 · HFMA Workforce Data 2025
Last Updated: March 31, 2026


