
Key Facts
- At Valley Diabetes & Obesity, an inbox triage agent cut daily inbox sorting from ~120 minutes to ~15 minutes over 10 months in production (Agentman customer data, 2026).
- The agent auto-routes ~80% of inbound fax, email, and voicemail, and the practice has recovered $50K+ from buried items — roughly $63K per physician per year in recaptured value (Agentman customer data, 2026).
- Across 10 months: zero missed referrals and zero expired prior-authorization windows.
- Close to half (114 of 243) of a physician's weekly EHR in-basket messages are generated by the system itself, not a person (Health Affairs, 2019).
- As many as half of specialty referrals are never fully completed, with the consult note often never returning to the referring practice (CRICO/IHI, 2017).
An AI inbox triage agent reads every inbound fax, email, and voicemail before staff do, classifies each by type and urgency, and routes it to a named owner. At Valley Diabetes & Obesity, it cut inbox sorting from two hours a day to fifteen minutes and recaptured $50K+ — but the bigger finding was clinical signal quietly leaking out of the EHR into an unwatched fax pile.
For years, a patient's insulin refill request landed exactly where it was supposed to: inside our EHR, in the refill queue, where a medical assistant sees it the same day. Then one of the dispensing pharmacies changed something, and the same reminder started arriving as a fax instead. Nobody told us. It just showed up in the fax pile one morning, looking like every other fax — a cover sheet and a number. We turned the agent on to clear a pile. That is not what it ended up doing.
Table of Contents
- What is an inbox triage agent, and what does it do for a medical practice?
- What was hiding in the inbox that 12 categories missed?
- How does an inbox triage agent get smarter every time it fails?
- Why is clinical signal leaking out of the EHR into the fax pile?
- What are the measurable results after 10 months?
- Is this only a Valley Diabetes problem, or does every practice carry this inbox?
- Frequently Asked Questions
What is an inbox triage agent, and what does it do for a medical practice?
An inbox triage agent is software that reads every inbound fax, email, and voicemail as it arrives, classifies each message by type and clinical urgency, and assigns it to a specific person rather than a shared queue. We deployed one at Valley Diabetes & Obesity, an independent specialty practice, in January 2026 to clear the morning fax pile — 47 faxes before 8 a.m., two hours of sorting before the doors opened.
The headline numbers held. Inbox sorting dropped from about 120 minutes a day to 15. Roughly 80% of inbound messages route themselves. But the part worth telling another practice owner about was never the 80% the agent handled cleanly — it was the 20% it could not place, and what that 20% turned out to be hiding.
"We didn't fix the fax pile by hiring. We gave it to something that reads every page, asks for help when it doesn't know, and remembers the answer."
— Sachin Gangupantula, FACHE, VP of Practice Operations at Valley Diabetes & Obesity and Co-founder of Agentman
What was hiding in the inbox that 12 categories missed?
When we went live, the agent launched with 12 classification categories. We thought that covered our inbox. It did not. Over 10 months, staff kept hitting clinically important messages that fit none of the original twelve — because a fax that belongs to no category is a fax nobody opens.
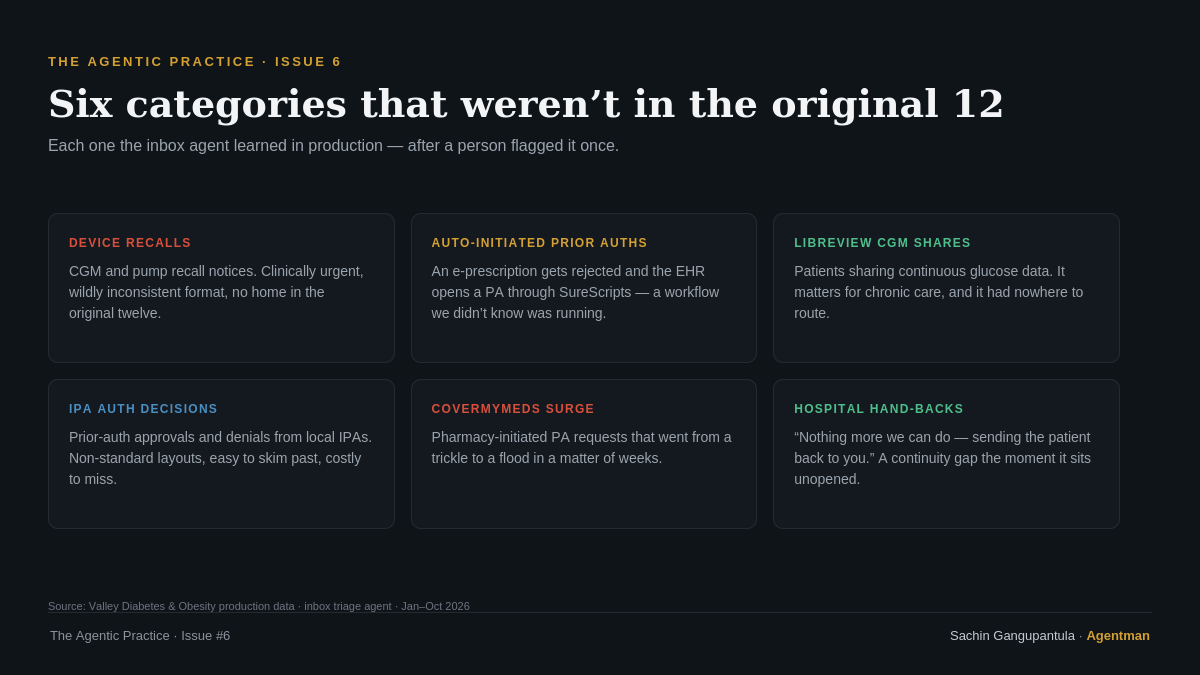
Here is what was actually hiding in the pile:
- Device recalls. Manufacturer notices on CGMs and insulin pumps — clinically important, wildly inconsistent in format, invisible to a generic "fax" bucket.
- Self-generated prior-authorization tasks. When an electronic prescription is rejected, our EHR's SureScripts integration appears to open a prior auth on its own. We did not know that pathway existed until the agent surfaced the tasks. A prior authorization agent only adds value if someone finishes what the system starts.
- LibreView CGM data shares. Patients sharing continuous glucose data with us — directly relevant to chronic-disease management, with no home in the original twelve.
- IPA prior-auth approvals and denials. Non-standard layouts from local independent practice associations, easy to skim past, and the difference between a paid claim and a write-off.
- A surge of CoverMyMeds PA requests. Not a new category so much as one that went from a trickle to a flood in weeks — and a fixed-headcount front office cannot absorb that kind of jump before things slip.
- Hand-backs from referral hospitals. A letter from a tertiary center saying there was nothing more they could do and the patient was coming back to us. If it sits unopened for two days, the patient assumes the hospital still has them, the hospital assumes we do, and for those two days no one does.
None were in the original twelve, and every one matters. We only found them because something was finally reading every page instead of a person triaging by cover sheet at 7:45 a.m.
How does an inbox triage agent get smarter every time it fails?
The agent improves through a closed feedback loop: every message it cannot classify goes to a visible "needs review" bucket, a person resolves it and names it as a new category with a priority, and that definition is written back into the agent's skill. The next message of that kind routes on its own.
This is the part most automation pitches skip. The category list did not stay frozen at twelve — it grew, shaped by what walked in the door rather than by what we guessed in December. The agent in month ten recognizes message types that had no category in January, because the people closest to the inbox taught it, one miss at a time.
The mechanism matters beyond one practice. A definition written the first time we saw an IPA denial is not a one-off fix for one fax — it is a skill. And a skill, once written, does not have to stay in one practice's inbox; it can travel to the next practice that sees the same message type. That is how a back-office automation platform compounds: each practice's hardest 20% becomes the next practice's pre-solved category.
Why is clinical signal leaking out of the EHR into the fax pile?
Structured clinical events are quietly migrating out of the EHR and into unstructured channels like fax, and no one is deciding that it should happen. The cleanest example: a patient's insulin refill request that used to arrive as a structured EHR refill-queue event started arriving as a fax after a dispensing pharmacy changed something on their end. Nobody announced it. It just showed up looking like every other cover sheet.
That refill now arrives twice — once through the EHR's SureScripts pipeline and once as a fax — because the integration never works 100% of the time. You cannot fully trust either channel alone, so a human used to reconcile both every morning.
Faxes also do not respect office hours. They arrive on weekends, holidays, and overnight — exactly when no one is watching the pile. An AHRQ-funded study found that time-sensitive alerts are less likely to be opened within 24 hours when they arrive on a weekend or land in an already-crowded inbox (Cutrona et al., AHRQ PSNet). The fax pile is not an administrative chore. It is where continuity of care slips when nobody is watching it closely enough.
What are the measurable results after 10 months?
After 10 months in production at Valley Diabetes & Obesity, the inbox triage agent cut sorting time by roughly 88%, auto-routes about 80% of inbound messages, and has recaptured more than $50K in buried work — while holding the clinical numbers at zero missed referrals and zero expired prior-auth windows.

| Metric | Before | After 10 months |
|---|---|---|
| Inbox sorting time | ~120 min/day | ~15 min/day |
| Messages auto-routed | 0% | ~80% |
| Value recaptured | — | $50K+ (≈$63K per physician/year) |
| Missed referrals | Untracked | 0 |
| Expired prior-auth windows | Untracked | 0 |
| Audit trail | Manual / none | Full trail on every item |
The number worth watching is not the time saved — it is the two zeros, because that is the clinical result. Here is the mechanism under it, because a clean number with no mechanism is just a hope.
A new diabetes-care referral used to arrive as a fax, join the pile, and get worked only if the right person happened to open it with time to spare. Now the referral management agent parses it on arrival, prioritizes it, and assigns it to one named person — not a queue. From there the chain runs with a human at the single checkpoint that needs judgment: the agent reads the attachments, flags what is missing (a chart note the PCP did not send, a lab the patient still owes), then triggers the eligibility verification agent; once eligibility lines up, it hands off to the prior authorization agent to draft the PA. Staff reviews and submits. Nothing fires into a payer unsupervised, and nothing sits in a pile waiting to be noticed.
Is this only a Valley Diabetes problem, or does every practice carry this inbox?
Every independent specialty practice carries a version of this inbox — the data says it is not a single-practice problem. The clearest evidence is on the EHR side, before fax even enters the picture.

| Finding | Source |
|---|---|
| Close to half (114 of 243) of a physician's weekly in-basket messages are system-generated, not from a colleague or patient | Health Affairs, 2019 |
| As many as half of specialty referrals are never fully completed; the consult note often never returns to the referring practice | CRICO/IHI, 2017 |
| Time-sensitive alerts are less likely to be opened within 24 hours when delivered on weekends or into a crowded inbox | Cutrona et al., AHRQ PSNet |
In-basket volume is one of the strongest predictors of physician burnout we have, and referral leakage is a direct revenue and continuity-of-care risk. On a panel the size of ours, half of specialty referrals going uncompleted is up to 20 patients a month you assume are handled who may not be. If you are sorting fax, email, and voicemail by hand, the filing backlog is the least of it — you are carrying clinical exposure you cannot see, because the person who would surface it is the same one sorting 47 faxes before the first patient walks in.
Related Entities
This account sits inside Agentman's broader work on agentic back-office automation for independent specialty medical practices under the product name MedMan. The inbox triage workflow hands off directly to the referral management agent, the eligibility verification agent (priced at $0.50 per check versus the $6.72 CAQH ProView benchmark), and the prior authorization agent, with the denial management agent picking up IPA approvals and denials surfaced from the pile. The work spans revenue cycle management (RCM) for specialty verticals including diabetes & obesity, wound care, and vein care, with reference customers Valley Diabetes & Obesity, Rosen Vein Care, and Heritage Wound Care.
Frequently Asked Questions
What is an inbox triage agent in a medical practice?
An inbox triage agent is software that reads every inbound fax, email, and voicemail as it arrives, classifies each message by type and clinical urgency, and routes it to a named staff owner instead of a shared queue. It replaces manual cover-sheet sorting and flags time-sensitive items such as referrals and prior authorizations.
How much time does an inbox triage agent save a specialty practice?
At Valley Diabetes & Obesity, the agent cut daily inbox sorting from about 120 minutes to about 15 minutes over 10 months — roughly an 88% reduction — while auto-routing approximately 80% of inbound messages and recapturing more than $50K in buried work.
How does an inbox triage agent handle messages it cannot classify?
Unrecognized messages go to a visible "needs review" bucket owned by a person rather than disappearing into the pile. Staff resolve the message, name it as a new category with a priority, and that definition is written back into the agent's skill so the same message type routes automatically next time.
Why are clinical messages arriving by fax instead of through the EHR?
Structured EHR events such as insulin refill requests can migrate to fax when a pharmacy or integration changes on its end, often without notice. Because EHR and SureScripts pipelines do not deliver reliably 100% of the time, the same message can arrive twice — once electronically and once by fax — requiring reconciliation.
Does an inbox triage agent submit prior authorizations on its own?
No. The agent prioritizes the referral, flags missing documentation, and triggers the eligibility verification and prior authorization agents to draft the work, but a staff member reviews and submits. Nothing is sent to a payer without human review.
What to do next
Three takeaways for any independent specialty practice owner weighing this:
- The 80% an agent routes cleanly is not where the value is. The 20% it cannot place is hiding device recalls, self-generated prior auths, and hospital hand-backs — clinically important work no one is watching.
- Pick a system that learns from its misses. A "needs review" loop that turns each failure into a reusable skill is what moved us to zero missed referrals over 10 months.
- Treat the fax pile as clinical exposure, not an admin chore. Continuity of care slips in the seam between systems — and the person who would catch it is the one sorting faxes at 7:45 a.m.
If you run an independent specialty practice and want to see how an inbox triage agent and the MedMan agent suite would handle your inbox, talk to us.
Sources
- Tai-Seale M, et al. "Physicians' Well-Being Linked To In-Basket Messages Generated By Algorithms In Electronic Health Records." Health Affairs, 2019. https://www.healthaffairs.org/doi/10.1377/hlthaff.2018.05509
- CRICO / Institute for Healthcare Improvement. "Closing the Loop: A Guide to Safer Ambulatory Referrals in the EHR Era," 2017. https://www.rmf.harvard.edu/podcasts//2018/closing-the-loop-3/
- Cutrona SL, et al. "Primary Care Providers' Opening of Time-Sensitive Alerts Sent to Commercial Electronic Health Record InBaskets." J Gen Intern Med, 2017 (AHRQ PSNet). https://psnet.ahrq.gov/issue/primary-care-providers-opening-time-sensitive-alerts-sent-commercial-electronic-health-record
What's the most clinically important thing you've ever found buried in your fax, email, or voicemail pile after the fact? Hit reply and tell me — the insulin refill above still bothers me.
Sachin Gangupantula, FACHE, MBA, CDH-E — VP of Practice Operations, Valley Diabetes & Obesity; Cofounder, Agentman
The Agentic Practice publishes when the practice lets me write it.


